Iveric Bio Announces Positive Topline Data from Zimura GATHER2 Phase 3 Clinical Trial in Geographic Atrophy

Iveric bio announced positive topline results from GATHER2, the company’s second phase 3 clinical trial of Zimura (avacincaptad pegol), a novel investigational complement C5 inhibitor, for the treatment of geographic atrophy (GA). GATHER2 met its prespecified primary endpoint of mean rate of growth (slope) in GA area at 12 months with statistical significance and a favorable safety profile.
“We are thrilled to see for the first time an investigational therapy with a statistically significant reduction in the rate of GA progression at the 12-month primary endpoint across two phase 3 clinical trials,” Glenn P. Sblendorio, Chief Executive Officer of Iveric Bio, said in a company news release. “The results from GATHER1 and GATHER2 and our Special Protocol Assessment with the FDA provide the basis for an NDA, which we are planning to submit by the end of first quarter of 2023. We look forward to engaging with the FDA throughout the review process. I want to thank the many patients, physicians and their staffs for their participation in the Zimura clinical program along with the employees of Iveric Bio for their dedication to achieve this important milestone.”
Safety Overview
In GATHER2, there were no events of endophthalmitis, no intraocular inflammation events, and no ischemic optic neuropathy events through month 12. The most frequently reported ocular adverse events were related to the injection procedure.
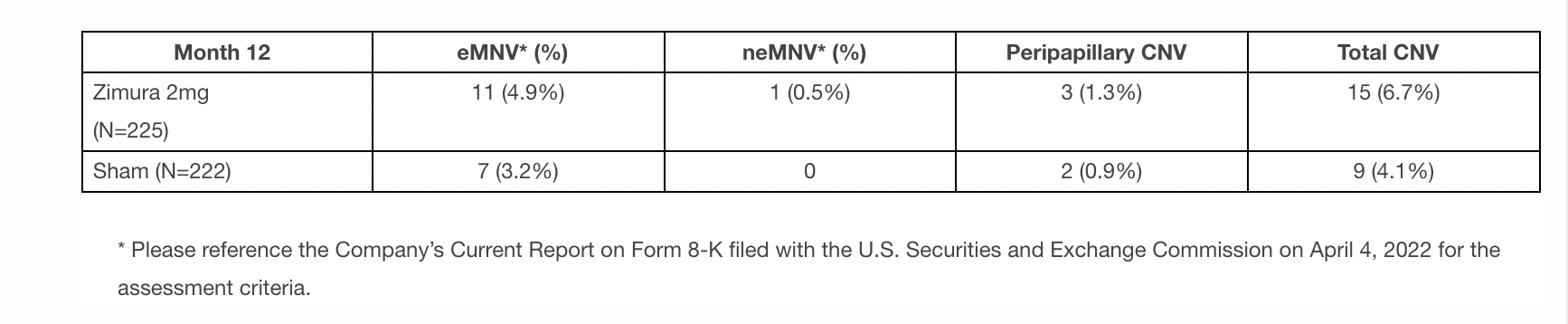
The incidence of choroidal neovascularization (CNV) in the study eye through month 12 was 15 patients (6.7%) in the Zimura 2 mg group and 9 patients (4.1%) in the sham control group. Similar to GATHER1, the company’s first phase 3 clinical trial of Zimura in GA, an independent masked reading center assessed the CNV cases in GATHER2 at the 12-month timepoint for exudative macular neovascularization (eMNV) and non-exudative macular neovascularization (neMNV). The accompanying table summarizes this analysis:
Efficacy Overview
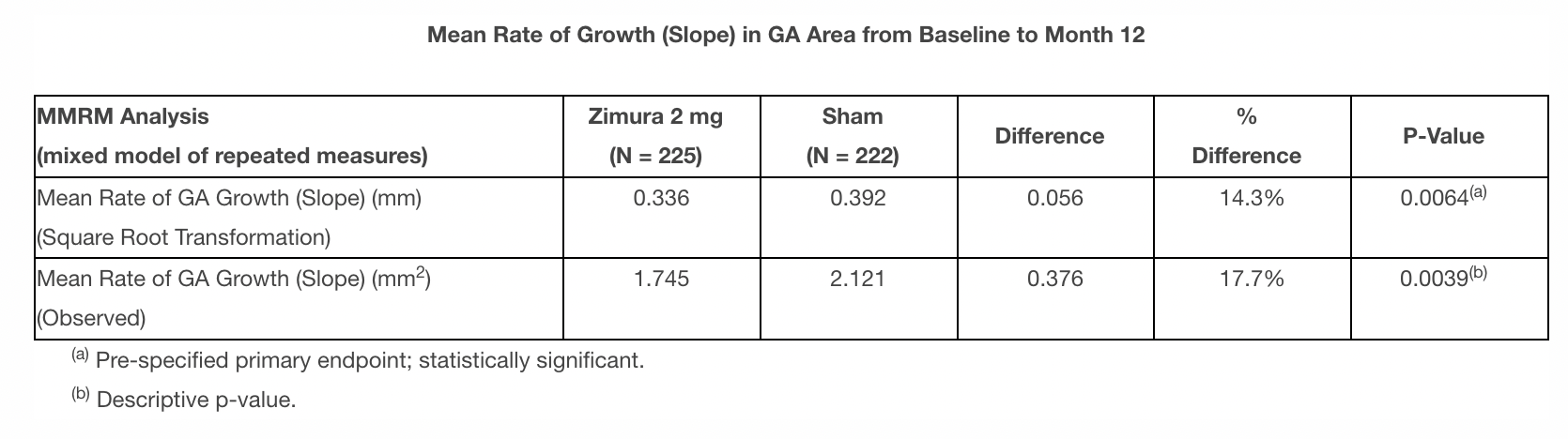
The prespecified primary endpoint, mean rate of growth (slope) in GA area over 12 months, was measured by fundus autofluorescence (FAF) based on readings at three time points (baseline, month 6, and month 12) and was calculated using the square root transformation of the GA area. The FAF images were assessed by an independent masked reading center. The company also analyzed the mean rate of growth (slope) in GA area without square root transformation (observed GA area). Detailed data for the primary endpoint and observed GA analysis are shown in the accompanying table:
 The company also analyzed the mean change in GA area from baseline to month 12 in GATHER2 using a point analysis, which was the prespecified primary endpoint in GATHER1. This analysis was performed based on FAF readings at the same three time points as the primary efficacy analysis (baseline, month 6, and month 12) using the square root transformation and the observed GA area. The results for the 12-month point analysis were consistent with the slope analysis. Details are provided in the accompanying supplement.
The company also analyzed the mean change in GA area from baseline to month 12 in GATHER2 using a point analysis, which was the prespecified primary endpoint in GATHER1. This analysis was performed based on FAF readings at the same three time points as the primary efficacy analysis (baseline, month 6, and month 12) using the square root transformation and the observed GA area. The results for the 12-month point analysis were consistent with the slope analysis. Details are provided in the accompanying supplement.
“Geographic Atrophy is a devastating and life-altering disease that severely impacts my patients, limiting their ability to drive, read and see the faces of friends and family,” Arshad M. Khanani, MD, MA, FASRS, Director of Clinical Research at Sierra Eye Associates, Reno, Nevada, said in the news release. “In addition to GATHER1, GATHER2 also meeting the primary efficacy endpoint is great news for patients suffering from geographic atrophy. Additionally, I am impressed with the safety profile of Zimura in both the GATHER1 and GATHER2 trials, as safety is critically important when evaluating potential treatment options.”
As part of the prespecified statistical analysis plan for GATHER2, the company also analyzed the mean rate of growth (slope) in GA area for Zimura 2 mg as compared to sham for prespecified patient subgroups based on baseline lesion size, baseline visual acuity, baseline autofluorescence pattern, age, and gender. Zimura 2 mg showed a reduction in the mean rate of growth (slope) in GA area for all analyzed subgroups.
The prespecified supportive endpoints in GATHER2 included the mean change in best corrected visual acuity (BCVA) and the mean change in low luminance best corrected visual acuity (LL BCVA) from baseline to month 12. For BCVA, a favorable trend for Zimura 2 mg was observed consistent with GATHER1. For LL BCVA, a favorable trend was not observed.
Additional Efficacy Analysis
In a post-hoc analysis of GATHER2, the company analyzed the reduction in mean rate of growth (slope) in GA area over 12 months for patients receiving Zimura by geographic region (U.S. versus rest of world). The reduction for patients receiving Zimura in the U.S. was 25.5% (descriptive P-value = 0.0037) using square root transformation and 32.0% (descriptive P-value = 0.0033) using observed GA area. Patients in the U.S., who accounted for 42.7% of enrolled patients, had a mean baseline lesion size that was 13% smaller than patients outside the U.S. The Company’s preliminary hypothesis for regional variation is disease stage. The company previously hypothesized that Zimura may be more impactful in earlier stages of GA, based on post-hoc analysis of the GATHER1 data. Consistent with this finding, patients in the US in GATHER2 may have been recruited at an earlier stage of the disease as evidenced by the smaller baseline lesion size. The company plans to continue to explore this hypothesis.
“We are delighted that both GATHER1 and GATHER2 have met their primary endpoint with statistical significance and a consistently favorable safety profile,” said Pravin U. Dugel, MD, President of Iveric Bio. “We believe Zimura has the potential to benefit GA patients by altering the natural course of their disease. With our GATHER2 SPA agreement, we plan to submit our NDA as expeditiously as possible. Our highest priority now is to make Zimura available to physicians and their patients as soon as possible.”
GATHER2 results are scheduled for presentation at the American Academy of Ophthalmology Annual Meeting (AAO 2022) beginning on September 30, 2022 in Chicago, Illinois.