



This Case Report is Interactive!
Strengthen your understanding of geographic atrophy by answering the challenge questions below.
Case Presentation
A 91-year-old man presented to our clinic in August 2022 with complaints of gradually decreasing vision in both eyes. He was previously diagnosed with geographic atrophy (GA) in both eyes. At the time of our examination, his medical history was positive for hypertension, chronic kidney disease, amyloidosis, dyslipidemia, and bladder and pancreas adenocarcinoma (both operated on and in complete remission/cure). Medications included apixaban (Eliquis, Bristol Myers Squibb), mirabegron (Betmiga), atorvastatin calcium (Lipitor, Upjohn), esomeprazole magnesium (Nexium, AstraZeneca), naltrexone, mirtazapine, and tafamidis. BCVA measured 6/9 OD and 6/60 OS. IOP was 10 mm Hg in each eye. Imaging captured at the time of the consultation demonstrated progression of the GA in both eyes compared to a prior visit in January 2019 (Figure 1). The patient was started on complement inhibition therapy (pegcetacoplan [Syfovre, Apellis]) in the left eye for three doses.
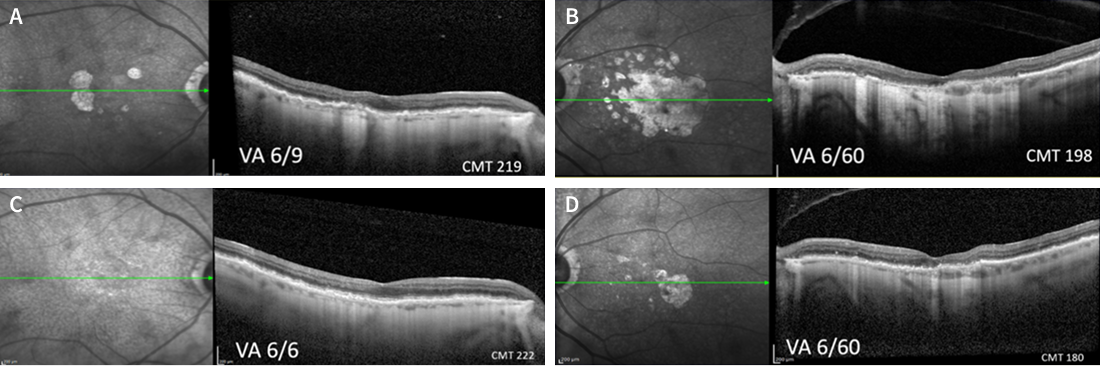
Figure 1. OCT images of the right eye (A) and left eye (B) of the patient in August 2022 showing progression of GA lesions compared to January 2019 (C, right eye; D, left eye).
OCT of the patient’s left eye in October 2022 showed no change of the GA and complement inhibition therapy was discontinued (Figure 2B). After this, each eye of the patient was monitored during routine visits in October 2022, February 2023, and April 2023 (Figure 2).
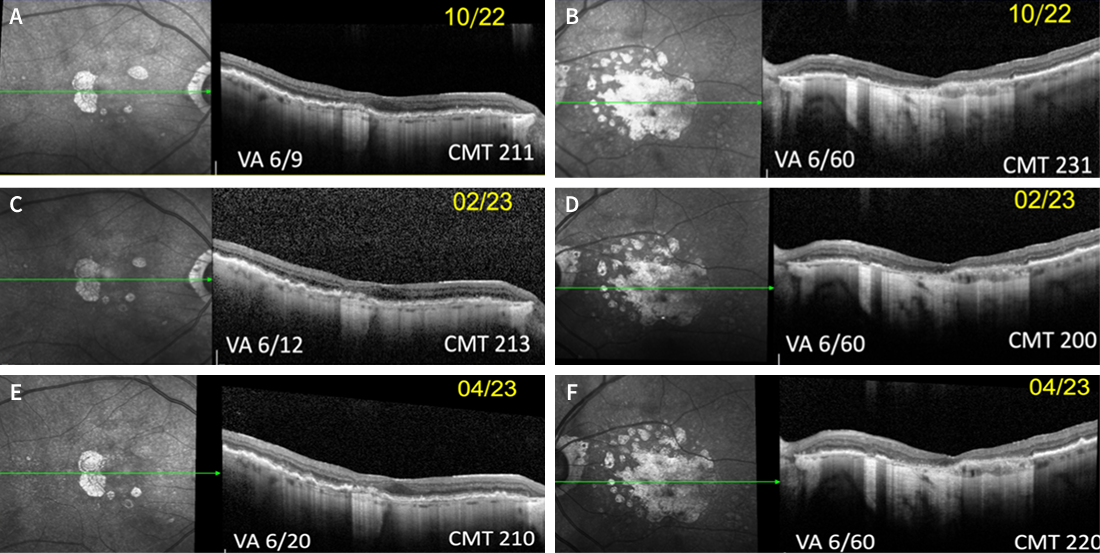
Figure 2. OCT images from routine monitoring visits of the patient over time. Figures A (right eye) and B (left eye) are from October 2022; figures C (right eye) and D (left eye) are from February 2023; and figures E (right eye) and F (left eye) are from April 2023.
Challenge Question 1/2
True or False: Neovascular age-related macular degeneration and geographic atrophy can co-exist in the same eye.
Answer the question above to reveal more case details.


Answer: A. True
When the patient presented in August 2023, the clinical examination and imaging in the right eye were consistent with new onset choroidal neovascularization (CNV; Figure 3). Correspondingly, the vision had deteriorated to 6/60. An intravitreal injection of aflibercept (Eylea, Regeneron) was administered as treatment. Imaging 1 month later showed partial resolution of the CNV, and no treatment was administered (Figure 4).
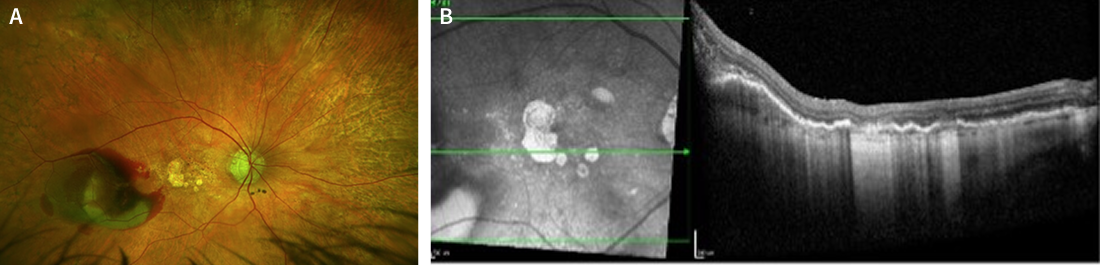
Figure 3. Color fundus photography (A) and OCT (B) of the patient’s right eye captured in August 2023 showed new onset CNV.
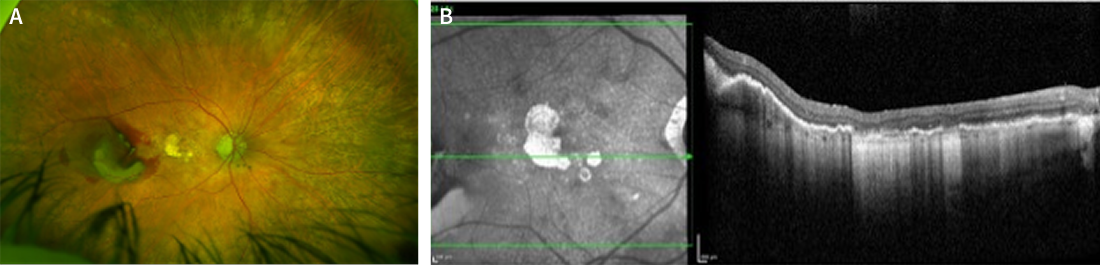
Figure 4. Color fundus photography (A) and OCT (B) of the patient’s right eye captured in September 2023, 1 month after administration of an intravitreal anti-VEGF agent, showed partial resolution of CNV.
Challenge Question 2/2
Which of the following is NOT true regarding geographic atrophy (GA)?
Answer the question above to reveal more case details.
Answer: C. GA is reversible and non-progressive
The patient was then followed in our clinic for routine monitoring of each eye in November 2023, January 2024, and March 2024 (Figure 5). As shown in Figure 5F, the patient developed sub-foveal bleeding in the left eye in March 2024. No treatment was offered for the left eye at that time, and the patient was directed to return in 1 month for continued monitoring. During this visit, in April 2024, the sub-foveal bleeding in the left eye demonstrated signs of resolution; however, for the right eye, the decision was made to restart anti-VEGF treatment. The patient was subsequently administered intravitreal aflibercept injections in April, May, and June 2024. OCT follow-up in the right eye is shown in Figure 6, and in the left eye in Figure 7.
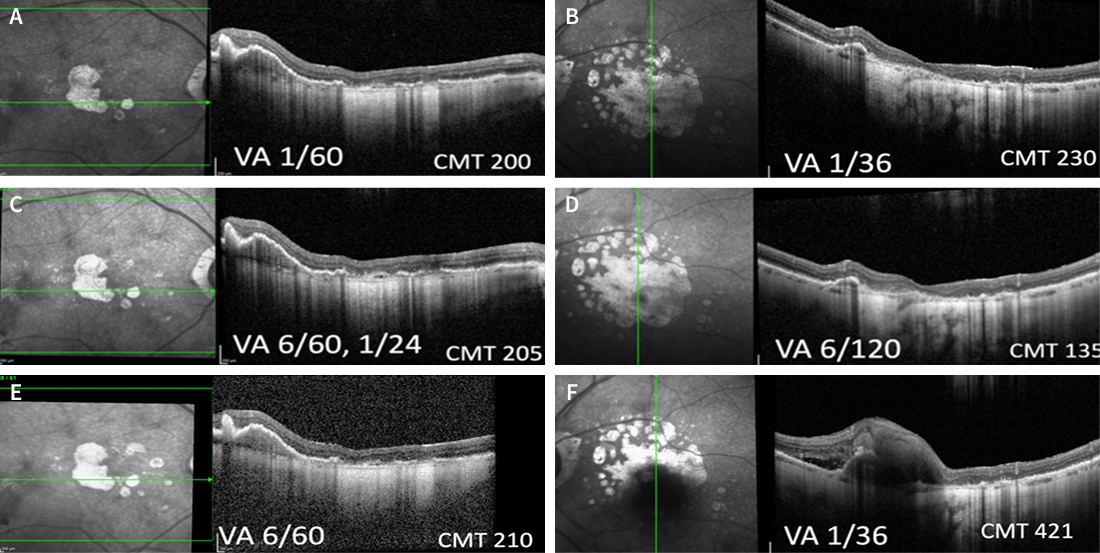
Figure 5. OCT images from routine monitoring visits of the patient over time. Figures A (right eye) and B (left eye) are from November 2023; figures C (right eye) and D (left eye) are from January 2024; and figures E (right eye) and F (left eye) are from March 2024.
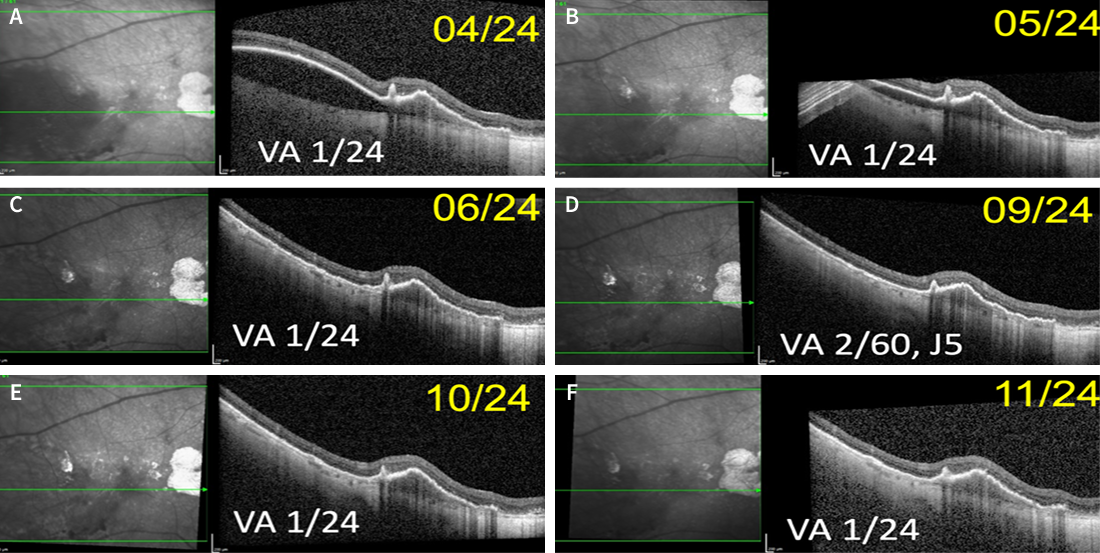
Figure 6. OCT follow-up of the patient’s right eye over time. Intravitreal aflibercept injections were administered in April, May, and June 2024.
This patient continues to be monitored closely in our clinic. In January 2025, the right eye experienced temporal rebleeding, which was partially resolved after three aflibercept injections (images not shown).
CAUTION: Spoilers ahead!
Finish the interactive case before reading the synopsis below.
Discussion
This is an interesting case of long-standing GA in a patient who developed CNV with bleeding and rebleeding in both eyes, possibly with the development of polypoidal lesions. Patients with GA should be monitored closely for the development of neovascular disease and treated accordingly.